ECR 2019 / C-2262
Idiopathic sclerosing encapsulating peritonitis: an unusual etiology of gastrointestinal obstruction
Congress:
ECR 2019
Poster Number:
C-2262
Type:
Educational Exhibit
Keywords:
Obstruction / Occlusion, Acute, Education, CT, Emergency, Abdomen
Authors:
P. Garcia Benedito1, A. M. Alcolado Jaramillo2, M. D. P. reyero lafuente3, E. VAN DEN BRULE4, A. PIAZZA DOBARGANES4, C. Gonzalez Hernando4; 1Mahadahonda/ES, 2Majadahonda/ES, 3Majadahonda, Madrid/ES, 4MAJADAHONDA-MADRID/ES
DOI:
10.26044/ecr2019/C-2262

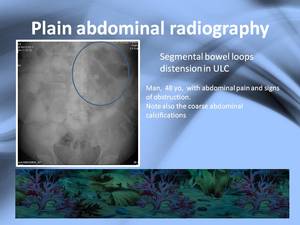
Fig. 6:
Plain abdominal radiography: bowel loop distensión in the LUC

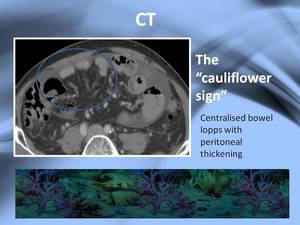
Fig. 7:
The cauliflower sign

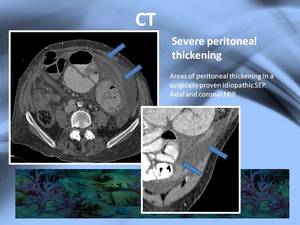
Fig. 8:
Peritoneal thickening

Fig. 9:
Peritoneal enhancement

Fig. 10:
Massive peritoneal thickening

Fig. 11:
Mesenteric calcifications

Fig. 12:
Loculated ascites

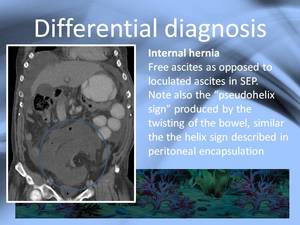
Fig. 13:
Internal herniation

Fig. 14:
Internal hernia resembling the "helix sign"

Fig. 15:
Peritoneal carcinomatosis

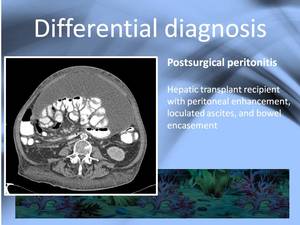
Fig. 16:
Post transplant peritonitis

Fig. 17:
MRI control of patient in fig. 16